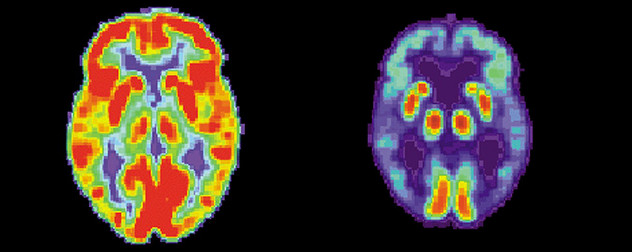
 PET scans of normal brain activity (left) and activity in a brain with Alzheimer's disease (right).
PET scans of normal brain activity (left) and activity in a brain with Alzheimer's disease (right).
Images courtesy the US National Institute on Aging, Alzheimer's Disease Education and Referral Center (healthy and Alzheimer's).With due respect to the adorable small ghosts and goblins who may ring our doorbells today, the specter that truly haunts millions of families around the globe is Alzheimer’s disease – and unlike those other phantoms, it will still be around tomorrow.
Yet a glimmer of hope emerged last week in dementia’s dark night. News broke that U.S. regulators will soon consider whether to approve the first drug meant to slow cognitive decline after it starts. This is a step that almost did not happen, and the drug in question – aducanumab, by Biogen Inc. – still may not be approved, either here or abroad. Even if it is, it remains to be seen how much the drug will cost. (It is safe to say the answer, at least in the United States, is likely to be “a lot.”) We also don’t know how readily insurers and government programs will agree to pick up the tab, or how effective the drug will actually be in real-world applications.
But it’s a start. The first treatment for Alzheimer’s is unlikely to be the last, even though it has taken many years, many dollars and many failures to get even this far.
In fact, aducanumab was thought to be one of those failures. Biogen halted two late-stage, Phase Three clinical trials, which were meant to determine the drug’s effectiveness, at the end of 2018 because the results were deemed to be unsuccessful. But upon further analysis, the data from one of those studies showed that at the highest dosages, the drug did significantly slow the rate of mental decline in patients who took it compared to those who received a placebo. And while the other study was still deemed to be unsuccessful, there were encouraging indicators in its data as well, The Wall Street Journal reported.
Biogen reportedly has been in discussions with the Food and Drug Administration since June. These discussions have centered on the possibly unprecedented step of reconsidering the results of those earlier trials to change the classification from failure to success, so the agency can determine whether to approve the drug as “safe and effective” for dementia treatment. The company says it plans to seek the FDA’s approval in early 2020.
Alzheimer’s already imposes enormous financial costs on society, along with equally heavy monetary and emotional costs on patients and their loved ones. The Alzheimer’s Association reported that the estimated annual cost for health care, long-term care and hospice care for Alzheimer’s patients is $290 billion. And that figure only represents the United States. The disease is a large and rapidly expanding problem in developed nations around the world, as the population ages and improved care reduces other causes of disability and mortality. Anyone who has seen Alzheimer’s up close – and this is a lot of us – knows how agonizing it is to lose loved ones who are physically still present but no longer able to meaningfully take part in their own lives. That is what often happens in late-stage Alzheimer’s.
The problem is not going to solve itself. On the contrary, it is likely to get worse. The number of Americans diagnosed with Alzheimer’s is projected to grow from 5.8 million in 2019 to 13.8 million by 2050.
There is virtually no medical hope for anyone already suffering from advanced Alzheimer’s. Although some patients may live up to 20 years with the disease, the typical lifespan after diagnosis is four to eight years. Right now, no pharmacological treatments can slow or stop the disease’s progress. Nonpharmaceutical therapies can sometimes improve patients’ quality of life, but they do not reverse neurological damage or change the disease’s ultimate outcome. As the global population ages, research into cures, or even effective treatment, takes on new urgency.
Aducanumab aims to slow the accumulation in the brain of beta amyloid, a compound of amino acids that is a major component of the plaques found in postmortem examinations of Alzheimer’s patients. There is no public indication yet that the drug can reverse or destroy these plaques, and there is still some question over whether the plaques are the cause or the result of Alzheimer’s. So aducanumab is not a potential cure for Alzheimer’s, but a potential treatment. Even then, other drugs targeting beta amyloid have previously proven ineffective.
If it works, or if similar but more effective compounds are developed behind it, aducanumab’s most significant impact could well prove to be in individuals who either have not developed Alzheimer’s yet, or who are in such early stages of the disease that it is not discernible in their behavior or in cognitive tests. We can already test for genetic markers that predict a genetic predisposition to early onset Alzheimer’s. Researchers are also trying to isolate biomarkers that can be administered in screening tests to identify others who might benefit from such a prophylactic treatment. Today, there are many diagnostic tools but no reliable test to catch the disease in its earliest stages. With a disease as complex and opaque as Alzheimer’s, developing a combination of effective testing and therapy is apt to be the shortest route to make a significant impact.
A true immunization against Alzheimer’s, or a reversal of moderate to advanced disease, seems to be significantly further off – if it happens at all in our lifetimes.
It may be that someday, people will see aducanumab as a primitive first attempt to vanquish the disease that has ruined millions of lives and haunted millions more. That would be a good thing. For now, it’s the only hope we have – assuming regulators agree it is better than nothing, and that someone is willing to pay for it.




Posted by Larry M. Elkin, CPA, CFP®
PET scans of normal brain activity (left) and activity in a brain with Alzheimer's disease (right).
Images courtesy the US National Institute on Aging, Alzheimer's Disease Education and Referral Center (healthy and Alzheimer's).
With due respect to the adorable small ghosts and goblins who may ring our doorbells today, the specter that truly haunts millions of families around the globe is Alzheimer’s disease – and unlike those other phantoms, it will still be around tomorrow.
Yet a glimmer of hope emerged last week in dementia’s dark night. News broke that U.S. regulators will soon consider whether to approve the first drug meant to slow cognitive decline after it starts. This is a step that almost did not happen, and the drug in question – aducanumab, by Biogen Inc. – still may not be approved, either here or abroad. Even if it is, it remains to be seen how much the drug will cost. (It is safe to say the answer, at least in the United States, is likely to be “a lot.”) We also don’t know how readily insurers and government programs will agree to pick up the tab, or how effective the drug will actually be in real-world applications.
But it’s a start. The first treatment for Alzheimer’s is unlikely to be the last, even though it has taken many years, many dollars and many failures to get even this far.
In fact, aducanumab was thought to be one of those failures. Biogen halted two late-stage, Phase Three clinical trials, which were meant to determine the drug’s effectiveness, at the end of 2018 because the results were deemed to be unsuccessful. But upon further analysis, the data from one of those studies showed that at the highest dosages, the drug did significantly slow the rate of mental decline in patients who took it compared to those who received a placebo. And while the other study was still deemed to be unsuccessful, there were encouraging indicators in its data as well, The Wall Street Journal reported.
Biogen reportedly has been in discussions with the Food and Drug Administration since June. These discussions have centered on the possibly unprecedented step of reconsidering the results of those earlier trials to change the classification from failure to success, so the agency can determine whether to approve the drug as “safe and effective” for dementia treatment. The company says it plans to seek the FDA’s approval in early 2020.
Alzheimer’s already imposes enormous financial costs on society, along with equally heavy monetary and emotional costs on patients and their loved ones. The Alzheimer’s Association reported that the estimated annual cost for health care, long-term care and hospice care for Alzheimer’s patients is $290 billion. And that figure only represents the United States. The disease is a large and rapidly expanding problem in developed nations around the world, as the population ages and improved care reduces other causes of disability and mortality. Anyone who has seen Alzheimer’s up close – and this is a lot of us – knows how agonizing it is to lose loved ones who are physically still present but no longer able to meaningfully take part in their own lives. That is what often happens in late-stage Alzheimer’s.
The problem is not going to solve itself. On the contrary, it is likely to get worse. The number of Americans diagnosed with Alzheimer’s is projected to grow from 5.8 million in 2019 to 13.8 million by 2050.
There is virtually no medical hope for anyone already suffering from advanced Alzheimer’s. Although some patients may live up to 20 years with the disease, the typical lifespan after diagnosis is four to eight years. Right now, no pharmacological treatments can slow or stop the disease’s progress. Nonpharmaceutical therapies can sometimes improve patients’ quality of life, but they do not reverse neurological damage or change the disease’s ultimate outcome. As the global population ages, research into cures, or even effective treatment, takes on new urgency.
Aducanumab aims to slow the accumulation in the brain of beta amyloid, a compound of amino acids that is a major component of the plaques found in postmortem examinations of Alzheimer’s patients. There is no public indication yet that the drug can reverse or destroy these plaques, and there is still some question over whether the plaques are the cause or the result of Alzheimer’s. So aducanumab is not a potential cure for Alzheimer’s, but a potential treatment. Even then, other drugs targeting beta amyloid have previously proven ineffective.
If it works, or if similar but more effective compounds are developed behind it, aducanumab’s most significant impact could well prove to be in individuals who either have not developed Alzheimer’s yet, or who are in such early stages of the disease that it is not discernible in their behavior or in cognitive tests. We can already test for genetic markers that predict a genetic predisposition to early onset Alzheimer’s. Researchers are also trying to isolate biomarkers that can be administered in screening tests to identify others who might benefit from such a prophylactic treatment. Today, there are many diagnostic tools but no reliable test to catch the disease in its earliest stages. With a disease as complex and opaque as Alzheimer’s, developing a combination of effective testing and therapy is apt to be the shortest route to make a significant impact.
A true immunization against Alzheimer’s, or a reversal of moderate to advanced disease, seems to be significantly further off – if it happens at all in our lifetimes.
It may be that someday, people will see aducanumab as a primitive first attempt to vanquish the disease that has ruined millions of lives and haunted millions more. That would be a good thing. For now, it’s the only hope we have – assuming regulators agree it is better than nothing, and that someone is willing to pay for it.
Related posts:
No related posts.